Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655




 Parasitology
Parasitology Specific Tests for Diet trials
Specific Tests for Diet trials
Bone I. Indications for bone biopsy. A. Bone tumours Do – particularly when classic radiographic…
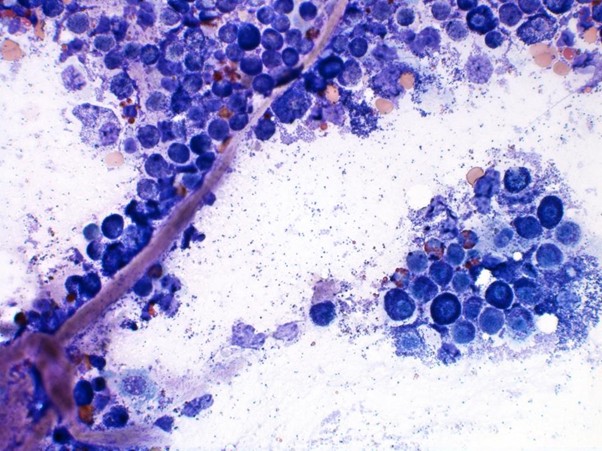
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More