Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655

Routine haematology, biochemistry and urinalysis are corner stones in the diagnosis
of hypercortisolism and will increase suspicion of the disease when performed in a
dog with suggestive clinical signs. Common changes include;
Haematology- stress leucogram, thrombocytosis, high reference interval or increased
red cell numbers.
Biochemistry- increased liver enzyme activities (ALP higher than ALT), hypercholesterolaemia, hypertriglyceridaemia, moderate bile acid increase, mild hyperglycaemia.
Urinalysis- Urine SG is typically <1.030, proteinuria, UTI (may have no signs and no
pyuria).
Confirmatory tests are undertaken when there is a high index of suspicion following clinical examination and routine laboratory testing. It does not seem appropriate to embark on expensive further testing in a dog with no clinical signs and limited routine laboratory test changes e.g. increased ALP activity alone.
ACTH Stimulation/Response tes
This test is used to help confirm hypercortisolism and is useful as a starting point of
therapy. This test is easy and quick to perform, it is specific (95%) but is less sensitive.
See table for how to perform the test. This is the test of choice when considering
iatrogenic hypercortisolism.
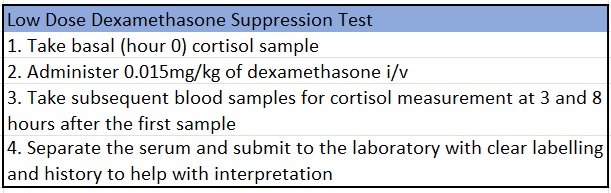
Low Dose Dexamethasone Suppression Test (LDDS)
A useful test to confirm diagnosis and may differentiate between adrenal and pituitary disease. This test takes 8 hours to perform and is sensitive but lacks specificity. It is a useful test to exclude hypercortisolism, but positive results can occur with other illness and stress. See table for how to perform test.
Urinary cortisol to creatinine ratio (UCCR)
A test that is used to screen for hypercortisolism but cannot differentiate between pituitary and adrenal gland disease when used in this format. The test is sensitive but lacks specificity. Urine must be collected at home, when the dog has not been to the clinic for at least 3 days and is not stressed. It is recommended to collect the first urine of the day (morning). A negative result makes hypercortisolism very unlikely.
Endogenous ACTH
Measurement of endogenous ACTH can be useful to distinguish between adrenal and pituitary gland disease following diagnosis of hypercortisolism. Dogs with hypercortisolism due to adrenal gland neoplasia should have very low eACTH and dogs with pituitary gland disease would be expected to have high reference interval or increased eACTH. The limitation of this test is that there are stringent sample handling requirements (see brochure), diagnostic imaging may provide the same answer. eACTH is not useful to confirm diagnosis of hypercortisolism due to its episodic secretion. It may be useful in cases where there are adrenal and pituitary masses.
Diagnostic Imaging
Abdominal ultrasound
Performing abdominal ultrasound is crucial in the diagnosis of hypercortisolism. These are often older animals and the potential for co-morbidities cannot be underestimated. Abdominal ultrasound allows for full investigation of the abdomen to eliminate the possibility of other disease that can mimic hypercortisolism e.g. liver disease, to look for co-morbidities e.g. kidney disease or neoplasia and to screen for diseases that can occur in association with hypercortisolism such as gall bladder mucocoele. With pituitary gland disease it is expected that there is bilateral adrenomegaly and typically with adrenal gland disease there is unilateral enlargement with atrophy of the contralateral gland. Adrenal gland masses can abut and invade the vena cava resulting in massive haemorrhage and thrombosis.
Computed Tomography
CT of the head is useful to confirm the presence of a pituitary mass or to determine its
size in the presence of neurological signs. This is an expensive test and is not routine
in the work up of dogs with hypercortisolism but does have its merits. CT of the
abdomen and chest would be considered for surgical planning and to screen for
metastasis in dogs with adrenal gland neoplasia.

Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
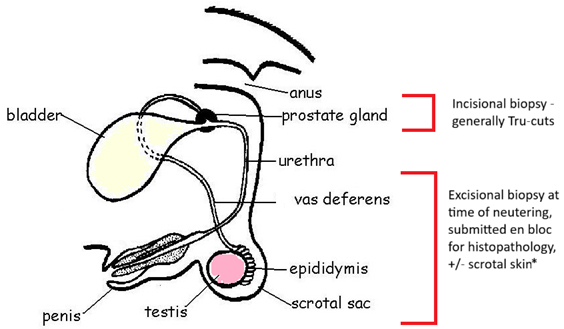
PART I – The Male Reproductive Tract I. Indications for biopsy/pathological evaluation The male reproductive…
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More