Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655


Anaemia may be encountered as the cause of dramatic presenting signs, or it may be an
unexpected clin path finding during investigations or even on pre-procedure screening tests.
Anaemia is present when there is a reduction in any one or more of haematocrit (HCT),
packed cell volume (PCV), red blood cell count, or haemoglobin (Hb) concentration.
Consider whether investigation of the anaemia is likely to be diagnostically useful.
Related to this is whether the anaemia is regenerative or non-regenerative; this classification
also helps to greatly narrow the differential list to be considered.
Sedation and general anaesthesia can lead to dramatic but artefactual reductions in haematocrit; one study quotes an average of 25% (Dhumeaux et al 2012), suggesting the effect could be due to drug-induced splenic relaxation.
There are no haematology machines that are optimised for the assessment of feline blood. Most struggle to count feline red and white cells accurately. Platelet clumping is almost the norm in cats, and the clumps are often about the size of a red blood cell, leading to inaccurate estimations of both red cell and platelet numbers. Sample quality and prolonged storage of samples may also adversely affect accuracy of results.
Some examples include:
Reticulocyte counts are mandatory to classify anaemia, but they are not provided by all inhouse
machines. Cats produce reticulocytes in two forms; aggregate, younger red cells
which are present for around 12 hours before maturing into punctate cells, with a smaller
amount of residual DNA. Aggregate reticulocytes are generally considered the best indicator of active regeneration, and the appropriate response to severe anaemia is a robust aggregate reticulocytosis. All veterinary haematology reports should provide an aggregate reticulocyte count for anaemic cats. However in mild anaemia, it is often the punctate reticulocytosis that is most pronounced, ideally a punctate count should be available on request, to avoid under-estimating the regenerative response in mild anaemia.
A pre-regenerative state reflects sampling in the per-acute stage of new anaemia, such that the bone marrow has not yet had time to respond to the effects of anaemia. Response takes around 3-5 days (generally the more rapid response will be seen with more dramatic red cell reductions), so strictly speaking anaemia cannot be classified as regenerative or nonregenerative until the blood is assessed for reticulocytosis after this time. That said, a cat presenting with severe anaemia and not in a collapsed or severely compromised state is likely to have had time for physiological adaptation, implying that a non-regenerative classification based on a single sample is correct.
There must be some blood loss or haemolysis.
With blood loss you may see low or low-normal proteins, although with acute, now ceased haemorrhage, or chronic low-grade haemorrhage, proteins will be rapidly resorbed or maintained by increased production, respectively.
The site of blood loss is usually fairly easily discovered with imaging, if it is not obvious from clinical examination. An exception to this would be diffuse, or small, gastrointestinal lesions leading to external blood loss.
In some cases, it may be necessary to seek a cause of increased bleeding tendency. In cats
this is generally rodenticide toxicity (prothrombin time is disproportionately prolonged) however there are a few hereditary clotting disorders (always worth a quick internet search if your patient is a pure-bred), and occasionally other acquired bleeding tendencies such as immune-mediated thrombocytopenia are a consideration.
Haemolysis generally causes a serum bilirubin increase, although in cats this is often not
dramatic, as haemolysis frequently has a pronounced extra-vascular component. Ghost cells (near-empty red cell membranes) may be seen.
There are many mechanisms of haemolysis, but most occur only rarely, and they can usually be easily excluded with signalment, history and basic clin path testing. Immune-mediated haemolytic anaemia (IMHA) is the most likely form of haemolysis in most cases, and contrary to long-held belief, it is commonly primary in cats (as in dogs). This does not mean it is not vital to exclude an underlying cause where possible (as this may alter treatment), but it should give reassurance that, if no cause is found, no cause is present. Spherocytes cannot be detected in cats as their red cells are already small (compared to dogs). Saline agglutination testing (SAT) may give a clue that there is an immune-mediated process but the test is poorly standardised and false positives and negatives are common. Coombs’ testing can be used to identify anti-red-cell antibody activity. Again, false negatives are possible; ideally the test is run at 4 and 37 degrees Celsius and room temperature (but this gets expensive). Note that that a positive result does not differentiate between primary and secondary IMHA.
Bone marrow dysfunction, either primary, or suppression from other disease. Various causes
can be excluded from history and simple clin path testing. Bone marrow analysis may be
required to identify the exact cause of other NRA, however, this step may not always alter
treatment options, despite giving greater interest to investigation and diagnosis.
Where a disease process may be primary or secondary, the list of possible underlying
conditions is similar or identical to that for IMHA. The contribution of M. haemofelis may be under-estimated in this setting. Additional considerations, particularly for aplastic anaemia, may be the effects of certain toxins, e.g. mycotoxins, estrogen toxicity. Note that a partiallydistinguishing feature of certain anaemias (B12 or folate deficiency, FeLV-related anaemia, and myeslodysplasia) is marked red cell macrocytosis.
Sometimes given its own category. This is not a particularly common mechanism of anaemia
cats, but it is worthy of mention since it is not always easy to diagnose. Typically, IDA occurs
after chronic, low grade, external blood loss, and the usual site for this is the gut. It could
occur from the urinary tract but this is very rare. Iron deficiency is sometimes difficult to
detect in cats, given that even when red cell parameters are normal, they have a greater
degree of anisocytosis and polychromasia than do dogs’, and, their red cells are already
smaller, such that detecting microcytosis and hypochromasia can be more difficult. In
addition, cats can be iron deficient without the classic morphological changes to red cells. Look for a dimorphic population of cells; normal, plus microcytic.
In the early stages, IDA will be regenerative. Over time, as the body is depleted of iron stores, the marrow is progressively less able to generate red cells, as it is lacking iron as a constituent part. Thus over time the anaemia becomes hypoproliferative, and eventually, even non-regenerative. Iron deficiency can look similar to anaemia of inflammatory disease (AID). Differentiation is not always easy, but it is usually possible; AID generally remains fairly stable over time, IDA is likely to progress. Iron status can be assessed via serum iron, saturation, and total iron binding capacity, but there can be a frustrating amount of discrepancy and overlap in the results which may reduce certainty of interpretation. Ferritin measurement is the most likely to differentiate, but very few laboratories are able to assess this. Bone marrow iron stores will be assessed as part of bone marrow analysis by a pathologist, should there be a need to sample the marrow, but false-negative results can occur due to patchy distribution of iron in feline bones. Trial treatment with iron (oral or parenteral) is a consideration; risk-benefit must be assessed, however severe complications such as anaphylaxis with parenteral iron do seem to be rare.

*Non-invasive tests with potential to differentiate
Haemoplasma infection
Black V, Adamantos S, Barfield D, Tasker S. Feline non-regenerative immune-mediated
anaemia: features and outcome in 15 cases. J Feline Med Surg. 2016 Aug;18(8):597-602
Chalhoub S, Langston CE, Farrelly J. The use of darbepoetin to stimulate erythropoiesis in
anemia of chronic kidney disease in cats: 25 cases. J Vet Intern Med. 2012 Mar Apr;26(2):363-9
Dhumeaux MP, Snead EC, Epp TY, Taylor SM, Carr AP, Dickinson RM, Leis ML. Effects of a
standardized anesthetic protocol on hematologic variables in healthy cats. J Feline Med Surg. 2012 Oct;14(10):701-5
Garden OA, Kidd L, Mexas AM, Chang YM, Jeffery U, Blois SL, Fogle JE, MacNeill AL, Lubas G, Birkenheuer A, Buoncompagni S, Dandrieux JRS, Di Loria A, Fellman CL, Glanemann B, Goggs R, Granick JL, LeVine DN, Sharp CR, Smith-Carr S, Swann JW, Szladovits B. ACVIM consensus statement on the diagnosis of immune-mediated hemolytic anemia in dogs and cats. J Vet Intern Med. 2019 Mar;33(2):313-334
Stanley EL, Eatroff AE. Hypocobalaminaemia as a cause of bone marrow failure and pancytopenia in a cat. Aust Vet J. 2017 May;95(5):156-160
Sylvane B, Prittie J, Hohenhaus AE, Tozier E. Effect of cross-match on packed cell volume after transfusion of packed red blood cells in transfusion-naïve anaemic cats. J Vet Intern Med. 2018 May;32(3):1077-1083
Tasker S. Haemotropic mycoplasmas: what’s their real significance in cats? J Feline Med Surg. 2010 May;12(5):369-81
Taylor S, Spada E, Callan MB, Korman R, Leister E, Steagall P, Lobetti R, Seth M, Tasker S. 2021 ISFM Consensus Guidelines on the Collection and Administration of Blood and Blood Products in Cats. J Feline Med Surg. 2021 May;23(5):410-432
Weiss DJ. Bone marrow pathology in dogs and cats with non-regenerative immune-mediated
haemolytic anaemia and pure red cell aplasia. J Comp Pathol. 2008 Jan;138(1):46-53
Weltman JG, Fletcher DJ, Rogers C. Influence of cross-match on posttransfusion packed cell
volume in feline packed red blood cell transfusion. J Vet Emerg Crit Care (San Antonio). 2014 Jul-Aug;24(4):429-36
Winzelberg Olson S, Hohenhaus AE. Feline non-regenerative anaemia: Diagnostic and treatment recommendations. J Feline Med Surg. 2019 Jul;21(7):615-631
Chikazawa S, Dunning MD. A review of anaemia of inflammatory disease in dogs and cats. J Small Anim Pract. 2016 Jul;57(7):348-53
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
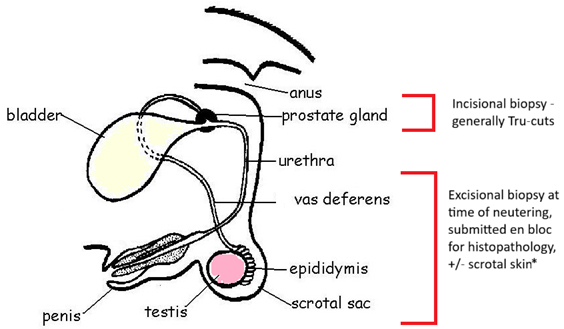
PART I – The Male Reproductive Tract I. Indications for biopsy/pathological evaluation The male reproductive…
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More