Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655


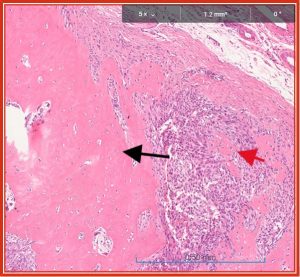
Fig. 1 Osteosarcoma. Black arrow indicates reactive bone progressing in maturity to left. Red arrow is tumour associated osteoid with irregularly spaced immature large osteoblastic cells. Tumour cells fill the medullary space between.
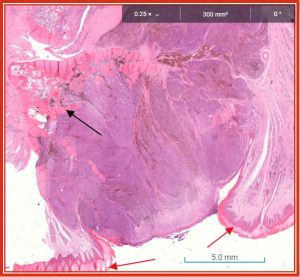
Figure 2. Melanoma of digit replacing the nail and most of the distal phalangeal bone (black arrow indicates bone remnants, red arrows displaced paronychial skin).
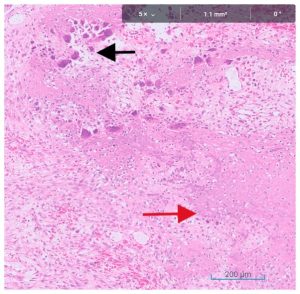
Fig 3. Fibrous osteodystrophy in a case of juvenile nephropathy. Black arrow indicates multinucleate osteoclasts indirectly stimulated by elevated parathormone responding to elevated phosphorus to resorb bone to correct calcium/phosphorus imbalance. Red arrow indicates abundant poor quality osteoid with irregularly spaced osteoblastic cells in an attempt to correct structural integrity. Compare with fig. 1 above where multinucleate osteoclasts remove bone in response to neoplastic infiltration and can also be part of the neoplastic population.
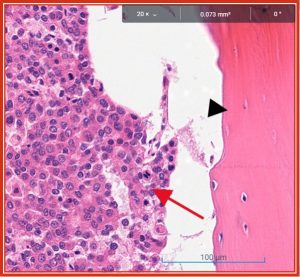
Fig. 4 Metastatic carcinoma (red arrow).
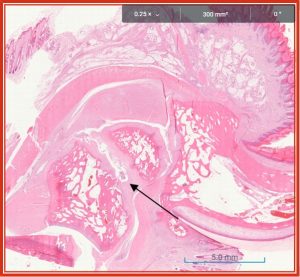
Fig. 5. Pseudo-arthrosis following malunion of fracture in middle digital bone
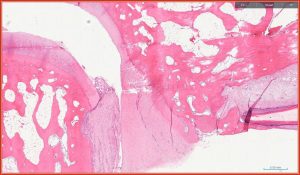
Fig. 6 Joint pannus infiltrating and replacing bone and cartilage on the left of the joint.
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
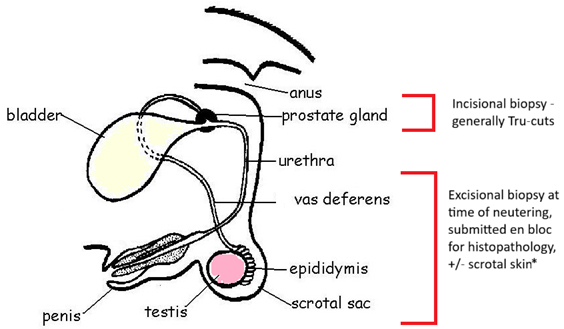
PART I – The Male Reproductive Tract I. Indications for biopsy/pathological evaluation The male reproductive…
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More