Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655

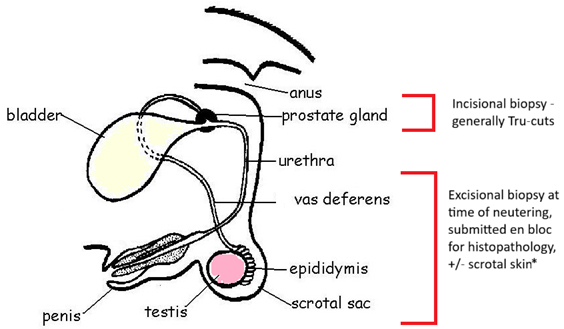
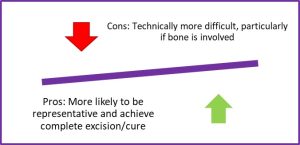
As with most organs and tissues, the two main types of biopsy are incisional and excisional. Incisional oral biopsies are most common, mainly because (i) they are easier to collect in this more awkward part of the body and (ii) they allow initial diagnosis and decision-making prior to undertaking anything more radical.
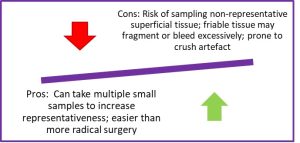 Fig 1. Incisional biopsies
Fig 1. Incisional biopsies
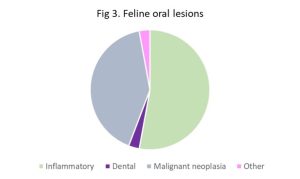
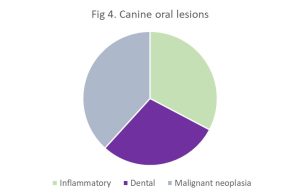
While oral lesions are common in dog and cat, the majority are benign and inflammatory. The pie charts below summarise the percentage of diagnosis in cats and dogs (Figs 3 and 4), derived from a recent review of such lesions2. While malignant neoplasms accounted for ~40% of feline oral lesions, this was mostly due to squamous cell carcinoma, the most common oral neoplasm in cats. More significantly, note that inflammatory lesions were even more common, accounting for around half the feline oral submissions in that study. In the same study, canine oral lesions were evenly distributed between inflammatory, odontogenic and malignant neoplasia. Malignant melanoma and fibrosarcoma were the top two canine oral malignancies but odontogenic neoplasia was more common compared to the cat, particularly fibromatous epulides of periodontal ligament origin (also known as peripheral odontogenic fibromas). While studies vary in fine detail, broad patterns are similar3.
It is not the purpose of this article to illustrate the full gamut of oral lesions but a select few below aim to highlight some specific points.
Figs 5A and 5C. Below are oral lesions from two different cats, both on the tongue. Figs 5B and 5D are high power views of 5A and 5C, respectively. Fig 5B is an eosinophilic granuloma (yellow arrow points to focus of collagenolysis caused by degranulating eosinophils and is rimmed by a granuloma). Fig 5D is a fibrosarcoma. These lesions are obviously very different in terms of likely behaviours, outcome and management, but they may appear similar grossly and even on low magnification.
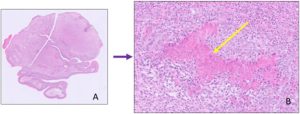 Fig 5A and 5B
Fig 5A and 5B
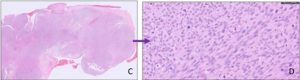
Fig 5C and 5D
Fig 6 illustrates how immunohistochemistry (IHC) may be required to reach a definitive diagnosis. Clockwise from top left: Standard haematoxylin and eosin (HE) at low magnification; HE at high magnification (no melanin!); IHC using Melan A, an antibody marker of melanocytes. This helped to confirm the suspected oral amelanotic melanoma.
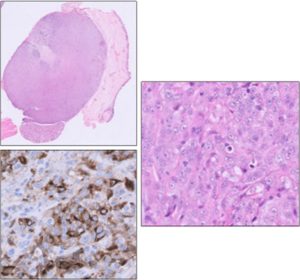
Fig 6. Use of IHC in diagnosis of oral neoplasia
The images below are of an oral lesion from a 12Y cat. While they comprise a florid polypoid epithelial lesion, with features consistent with chronic hyperplastic gingivitis, we could not conclusively exclude squamous cell carcinoma.
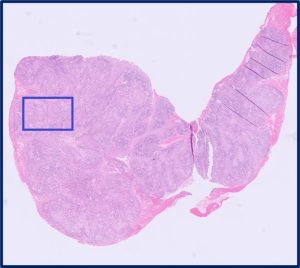
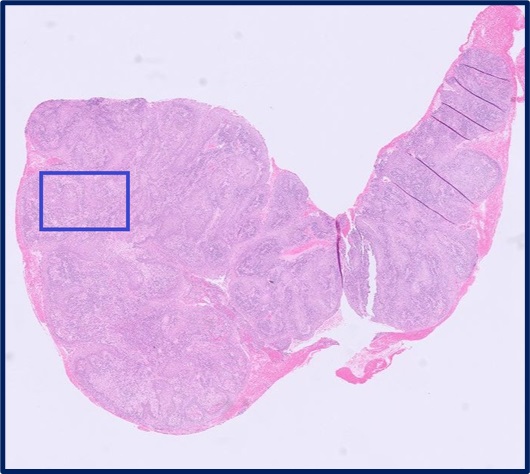
Appendix A: Low power image of the lesion – polypoid portion of gingival mucosa and subgingival stroma. 12Y DSH cat. Blue box in Appendix B below.
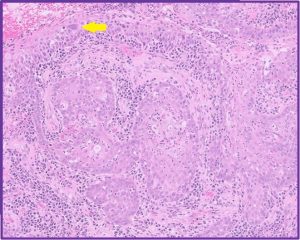
Appendix B: Higher power image of area in blue box (Appendix A above). While there are islands of squamous cells in the stroma, they are not particularly atypical and could be invaginations from the hyperplastic mucosal epithelium, rather than truly invasive neoplastic cells. However, the yellow arrow highlights an atypical surface epithelial cell that raises some suspicion of malignancy (or at least squamous cell carcinoma in situ, where the neoplastic cells are restricted to the mucosal epithelium and have not yet invaded). See higher power image of this cell in Appendix C.
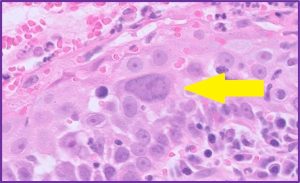
Appendix C: Very atypical surface epithelial cell in the gingival mucosa with atypically large nucleus and large nucleolus. Dysplasia secondary to inflammation can cause atypia but this is extreme even for that. The final diagnosis was marked chronic active, hyperplastic stomatitis with atypia. In cases such as this, close monitoring, radiographs and resampling as necessary are generally suggested.
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
PART I – The Male Reproductive Tract I. Indications for biopsy/pathological evaluation The male reproductive…
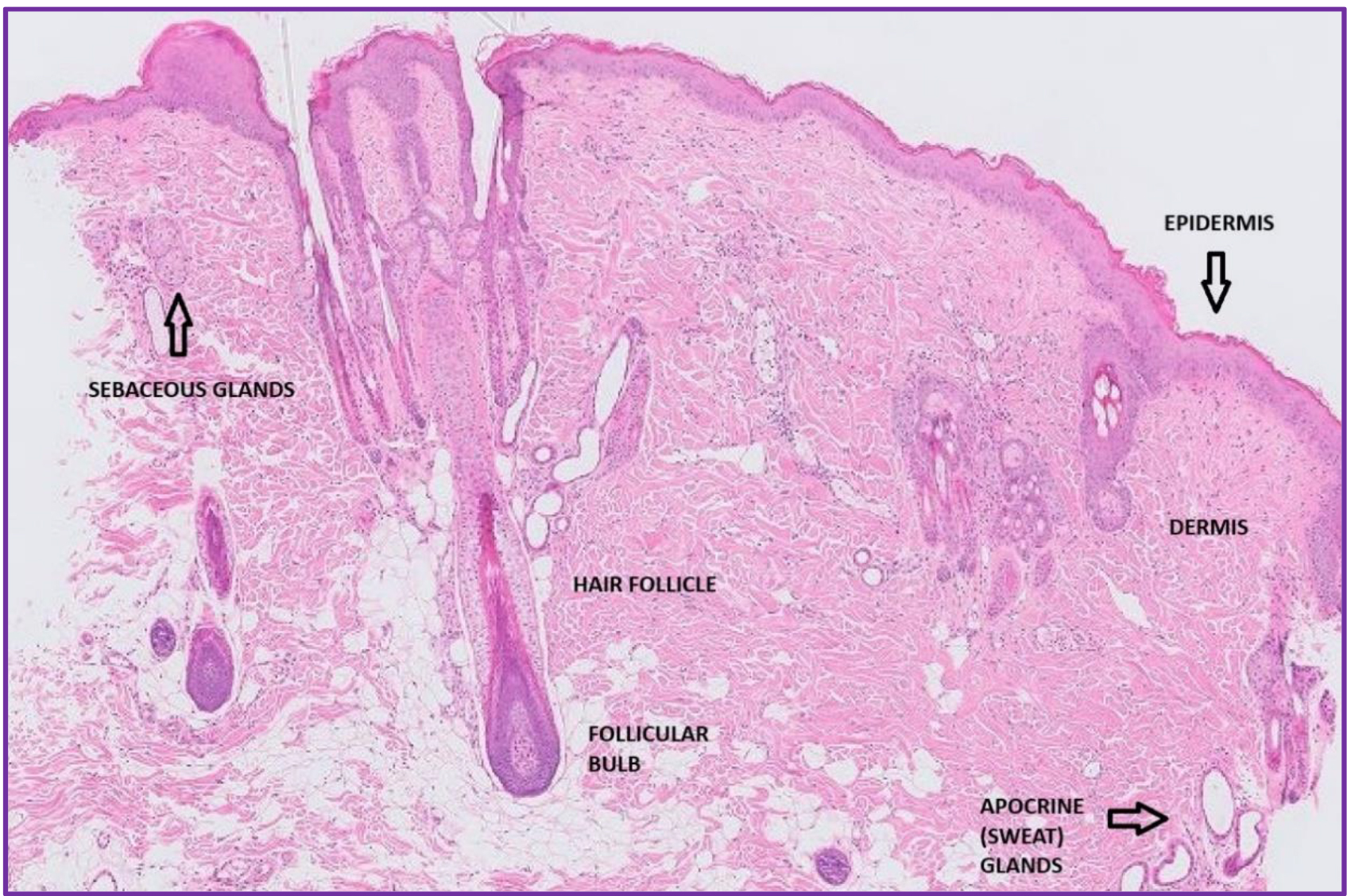
Organ of the month: Skin I. Indications for skin biopsy Skin biopsies account for a…
PART I – The Female Reproductive Tract I. Indications for biopsy/pathological evaluation As a reminder,…
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More