Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655
Our ordering platform is now closed, our sister company MiLab Diagnostics are now handling our consumable orders. If you have not received an invite for their platform please visit milab.store and submit a request, please ensure you populate all the fields on the request form.
Hello Colleagues
Our ordering platform is now closed, our sister company MiLab Diagnostics are now handling our consumable orders.
If you have not received an invite for their platform please visit milab.store and submit a request, please ensure you populate all the fields on the request form.
Thank you, Team Axiom.


Indications for gastrointestinal biopsy may be based on the clinical presentation of the animal, laboratory test results or other techniques such as imaging
Indications for GIT biopsy
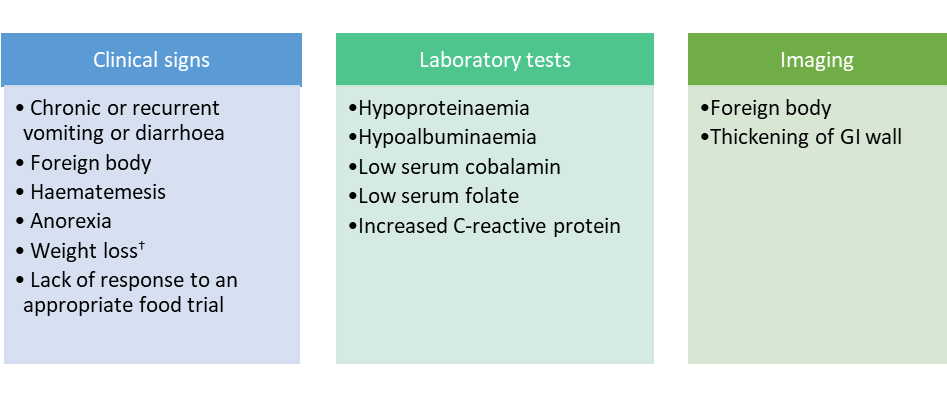
Table 1. Endoscopic biopsies
Fast and minimally invasive
AlLows direct evaluation of the GIT mucosa, particularly oesophagus, stomach, duodenum, ileum & colon
Allows potentially large numbers of samples to be taken at different levels of GIT
Samples are appropriate for histopathology as well as other techniques, such as immunohistochemistry, PARR and fluorescent in situ hybridisation (FISH)‡
Generally only captures mucosa and sometimes superficial submucosa, but not the wall
Lesions are often patchy in the GIT and this technique is better suited to more diffuse lesions
Cannot reach jejunum or distal duodenum in large dogs
Some samples are too hard to sample (e.g. carcinomas)
‡ Immunohistochemistry, PARR and FISH can be run on formalin fixed, paraffin embedded tissue
Table 2. Full-thickness biopsies
Any lesion can be sampled regardless of site, texture, size or consistency
More appropriate when evaluation of the intestinal submucosa and/or muscular wall is important, particularly for evaluation of neoplasia
May allow resection and cure of local disease
Allows assessment of the serosa and more of the GI tract, including less accessible areas (jejunum)
Samples are appropriate for histopathology as well as other techniques (see Table 1)
Much more invasive requiring abdominal surgery, hospitalisation and longer convalescence – leads to increased costs
Cannot see the mucosa
Slight risk of wound breakdown and peritonitis
Increased risk of post-operative morbidity
Example images of each type are present at the end
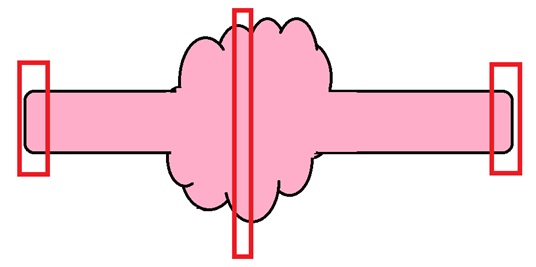
Most of the time, the enterectomy samples we receive are localised lesions detected at surgery, on palpation or via imaging, the aim being to achieve complete removal and potentially cure. Examples include areas of ulceration/perforation, neoplasms, other space-occupying lesions, and intussusception sites.
Fig 2 shows the general approach to processing such specimens.
More samples may be required if considering copper analysis and culture, in addition to histopathology. In such circumstances, five samples are considered “adequate”5.
Collect as much tissue as possible; place different sites in different pots and label them.
Best to avoid lobe tips as they may be less representative or even misleading.
Fig 2. Intestinal resection with mass. Red boxes depict areas sampled, allowing evaluation of margins.
Endoscopic samples: Sample stomach (fundus and pylorus), duodenum, ileum and colon depending on presentation. By taking eight good quality samples from each site, this will help to maximise diagnostic value, i.e. there will always be some samples that are not sufficiently deep, suboptimally oriented or artefactually crushed, but more numerous samples help to overcome this4.
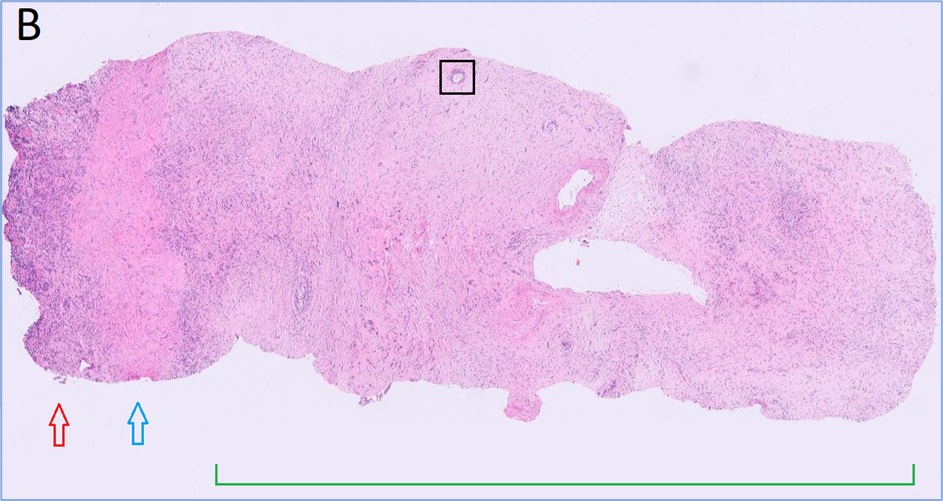
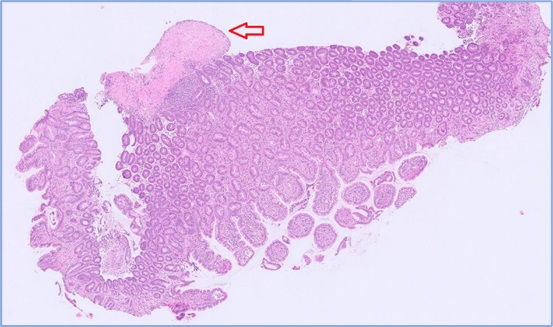
Full-thickness samples: These are the best samples to send if you are concerned about neoplasia or if there is suspicion of lesions in the submucosa or muscular wall. Many lesions are within the deep mucosa, crypts or submucosa so superficial samples may not be diagnostic. Adenocarcinoma of the GIT is often diagnosed based on invasive lesions in the submucosa or wall – endoscopic samples limited to the mucosa may miss the lesion (see Fig. 3, an example of invasive rectal adenocarcinoma).
How to send: Samples should be sent in 10% neutral buffered formalin. While samples can be shaken from the biopsy forceps directly into the formalin, studies have shown that better results are achieved by mounting the samples on a support medium, e.g. foam or cellulose acetate paper or filter paper5. They are also less likely to be overlooked. At our laboratory we can receive samples free floating in formalin, on foam, or on paper. Our preference is CellSafe6, a more secure tissue cassette with extra fine mesh. This sometimes comes with compartments so you can send multiple levels of GIT in the same cassette. Once samples are secured within the cassette, it is placed in a pot of formalin.
Please send different sites in different labelled pots. Stomach samples can go in the same pot unless you are concerned about a particular area in the stomach, e.g. you spot a lesion. Then you should send them separately labelled.
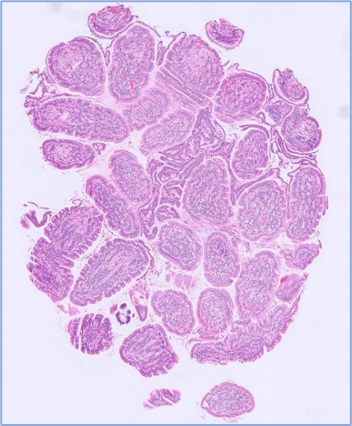
Fig 3. Rectal adenocarcinoma in a dog.

The following information is extremely helpful when we are assessing gastrointestinal biopsies:
Bone I. Indications for bone biopsy. A. Bone tumours Do – particularly when classic radiographic…
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
For receiving our news and updates in your inbox directly.

Manor House, Brunel Road, Newton Abbot, Devon, TQ12 4PB
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More