Email Us
admin@axiomvetlab.co.uk

admin@axiomvetlab.co.uk
(01626) 355655
Our ordering platform is now closed, our sister company MiLab Diagnostics are now handling our consumable orders. If you have not received an invite for their platform please visit milab.store and submit a request, please ensure you populate all the fields on the request form.
Hello Colleagues
Our ordering platform is now closed, our sister company MiLab Diagnostics are now handling our consumable orders.
If you have not received an invite for their platform please visit milab.store and submit a request, please ensure you populate all the fields on the request form.
Thank you, Team Axiom.

– Chronic cough
– Chronic increase in respiratory effort or tachypnoea
– Diffuse changes in lung fields on imaging, if there are associated clinical signs
– Poor anaesthetic stability
– Bronchospasm
– Pneumothorax
*NB these risks are inherent, associated more with the underlying disease process than the procedure
itself.
The patient should be anaesthetised, intubated with sterile endotracheal tube, placed in sternal or lateral recumbency (see below).
Put on the sterile gloves.
Measure the tube to the end of the rib cage to ensure it is long enough.
If the feeding tube distal ports are to the side, use the scalpel blade to cut the end of the tube off in a sterile manner to make it ‘end tip’ rather than ‘side tip’.
Fill appropriate syringes with warm sterile saline.
Ensure the patient is stable and asleep, with a high SpO2 reading (manual ventilate for a breath or two if needed).
Turn off the gaseous anaesthesia, squeeze the bag to empty it of the gas and disconnect the from the ET tube (* or use the capped port and do not need to disconnect).
Insert the sampling tube through the sterile ET tube and advance it until it will go no further
(presumably lodged in a bronchus).
Connect the saline filled syringe, rapidly instil the fluid, and immediately aspirate while an assistant performs gentle coupage.
If there is negative pressure, withdraw the tube slightly and re-aspirate. If the tube fills with air,
move the tube slightly, detach, expel the air and try again.
It is unusual to recover all of the fluid instilled. Remaining saline will be resorbed by the patient
without complication.
Remove the tube with the syringe still attached and ensure the tip is facing up on removal to prevent loss of fluid.
Insert the tip of the tube in to the plain universal container, expel the fluid from the syringe through the tube (flushing it) and then remove the syringe (keep tube in the universal container), fill it with air and once again attach to the tube and expel the air through the tube to remove any remaining fluid.
Repeat the procedure one more time collecting the sample in to the same universal container.
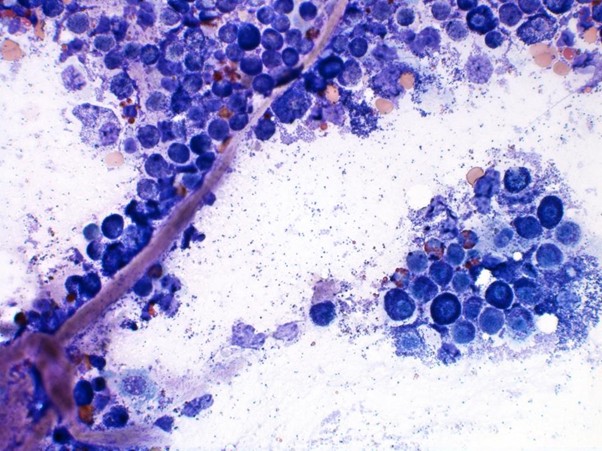
Once both samples have been collected use the 1ml syringe to remove a representative sample to place in to the EDTA container for cytology.
The last drops of the fluid from this syringe can be used to make 1-3 slides for microscopy, by lightly smearing a drop of fluid with another microscope slide and allowing this to dry.
Submit the samples for cytology and culture. PCR testing is often helpful where there is suspicion for an infectious cause (based on clinical findings, or subsequent to cytological description).
In case of complication:
Bone I. Indications for bone biopsy. A. Bone tumours Do – particularly when classic radiographic…
Reference Guide to Fine Needle Aspiration of Skin Lesions: A Practical and Diagnostic Cornerstone in…
Muscle I. Muscle biopsy In this blog, we turn to muscle biopsies, specifically skeletal muscle. …
Mammary Glands I. Indications for biopsy/pathological evaluation Mammary lesions are among the most common samples…
For receiving our news and updates in your inbox directly.

Manor House, Brunel Road, Newton Abbot, Devon, TQ12 4PB
The great explorer of the truth, the master-builder of human happiness no one rejects dislikes avoids pleasure itself because it is pleasure but because know who do not those how to pursue pleasures rationally encounter consequences that are extremely painful desires to obtain.
Read More